
Health
Special Report-UMTH: Looking at the Cancer Center Under Professor Ahidjo’s Led Management Team (3)

Special Report-UMTH: Looking at the Cancer Center Under Professor Ahidjo’s Led Management Team (3)
By: James Bwala
As a way to wrap up this piece, let me mention that the management team of Professor Ahmed Ahidjo is actively working to provide Nigerians seeking assistance with cancer treatment with the greatest possible care. The CMD has taken concrete action and made public statements to support the training of doctors who specialize in clinical oncology and related fields. If only to find water, the CMD might go anywhere and crack the rock. An official count of oncology or general surgeons in Africa could not be located after searching through reports on cancer-related topics. In 2010, a thorough analysis of the literature from sub-Saharan Africa (except from South Africa) on the state of surgery in the region indicated that there were just under two surgeons for every 100,000 people living there. For comparison, there were more than 35 surgeons in the same number in England.
As a result, surgery and anesthesia were performed—and are still performed—in many district hospitals by non-physicians who received special training for the job. The majority of oncologic surgery was carried out by general surgeons in referral hospitals. According to the study, the large-scale emigration of medical school graduates and the lack of surgically specialized programs in many African nations were the main causes of the low number of surgeons in the region.

Many Nigerians are now wondering how Professor Ahmed Ahidjo was able to reach the ground under his leadership in hospital management at the University of Maiduguri Teaching Hospital, which prides itself as the “Centre of Excellence”. We also made inquiries. How many radiation facilities are currently operating in Africa? Are these covering the need for cancer therapy sufficiently? How many additional units will be necessary? And so on. Radiotherapy plays a major role in the curative arsenal of a cancer unit.
When examining the primary therapeutic approaches utilized to treat cancer patients, it was discovered that surgery was the primary approach in 49% of cases, radiation was the primary approach in 40% of cases, and chemotherapy was the primary approach in the remaining 11% of cases. According to a survey conducted in the high-income nation of Australia, little more than 52% of cancer patients required radiotherapy as part of their treatment regimen. However, it is believed that up to 60% to 70% of new patients in low-income countries require radiotherapy due to a lack of surgical treatments and the high proportion of advanced-stage tumors that call for palliative care.
In light of this, only 277 external-beam radiation devices were registered for the African continent in the IAEA’s Directory of Radiation Centers in 2010. Of them, two nations—South Africa and Egypt—accounted for 60%. In addition, of the 52 nations surveyed, 29 African nations did not offer radiotherapy to cancer patients. According to the IAEA, more than 700 additional teletherapy machines would be needed on the continent given the estimated 713,206 cancer cases per year in Africa (according to GLOBOCAN 2008) and the fact that one teletherapy machine can treat 450 new cases of cancer annually.
There are currently no specific statistics available on the accessibility of chemotherapy drugs across the continent of Africa. In 2012 and 2018, an assessment of the situation in sub-Saharan Africa was made, which revealed a number of issues. All 22 of the chemotherapeutic medications on the WHO essential list are probably imported into the region, most of them as generics, but not all of the medications are always available. It is assumed that there is a severe scarcity of systemic anticancer drugs based on extrapolating the status of other critical medications on the WHO list, whose availability was proven to cover barely half of the demand. The scientists also discovered that, on average, the prices of pharmaceuticals in Africa were between 2.7 and 6.1 times higher than the prices used as international benchmarks. Finally, they calculated that there aren’t enough certified medical professionals available to give chemotherapy.

The situation is best illustrated by a review of the pharmaceuticals accessible for cancer therapy at a cancer center in Tanzania; over the time period studied, only about 50% of the specified medicines were available, which resulted in more than 70% of patients not receiving adequate therapy. The expense of purchasing the medications privately ranged from 1 to 7 months’ worth of income. Only a few patients were able to pay because the majority of them lacked insurance. Services in anatomic and clinical pathology are essential for cancer prevention. Pathology studies provide evidence for each stage of the diagnostic process, including the detection of malignant disease, diagnosis, staging, planning the surgical procedure, assessing management complications, and monitoring the outcome of treatment.
Furthermore, pathologic confirmation of the diagnoses is required for the cancer registry data to be taken seriously. For realistic planning of cancer control measures, this final input is crucial. Although there are no official statistics on the state of pathology services in Africa, the information that is currently available indicates a serious shortage in both quantity and quality. According to a 2012–20 informal assessment of pathology capacity in sub-Saharan Africa, the number of pathologists in the region was roughly 10% lower than that of specialists in fields equivalent to pathology in high-income nations.

The African Pathologists Summit, held in 2013 in Dakar, also noted the lack of pathologists and technicians, the poor state of the equipment, the inadequate infrastructure, and the difficulties in getting laboratory supplies. An extensive assessment of cancer prevention in Africa was just released. The analysis reiterates that most malignancies in Africa with the highest incidence rates can be prevented. For instance, human papillomavirus vaccination and other population screening techniques can prevent cervical cancer; hepatitis B vaccination can prevent liver cancer; eliminating malaria and HIV infections can lower the risk of Burkitt lymphoma (HIV is also the primary cause of the high incidence of Kaposi’s sarcoma); and limiting sun exposure can prevent skin cancer.
The investigation did discover that the region’s preventative measures are insufficient. According to the literature, not enough people are aware that cancer exists as a disease, that it has risk factors and manifestations, and that there are methods for preventing and treating it. Additionally, a number of cultural aspects make it difficult to use preventative strategies developed for other sociocultural contexts. The infrastructure and staff in place to enable mass prevention efforts in the health sector are insufficient. Although vaccination programs against the human papillomavirus and the hepatitis B virus are conducted on the continent, they are mostly supported by funding from outside organizations like the United Nations or the Global Alliance for Vaccines and Immunizations.

Governments lack the motivation to fully commit to the fight against cancer, and the majority of nations lack national cancer registries, which would provide accurate information on the scope and character of the issue. In a 2009 analysis of the global burden of cancer, the Economist Intelligence Unit discovered a significant gap between the cancer costs on the African continent, which accounted for just 0.3% of the global costs, and the continent’s share of the world’s new cases of cancer, which accounted for 6.4% of the world’s annual total. The amount spent on cancer treatment is disproportionately low in Africa since the majority of cancer costs are represented by medical expenditures (medications, medical procedures, charges for hospitalization, and outpatient visits).
READ ALSO: https://newsng.ng/the-plight-of-farida/
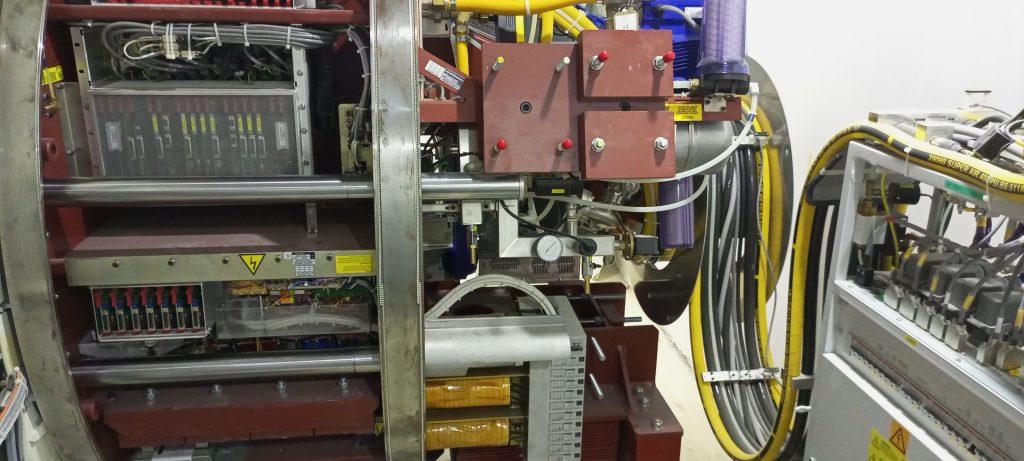
We were able to see the wider picture of the efforts being made by Professor Ahmed Ahidjo, Chief Medical Director of the University of Maiduguri Teaching Hospital, and his management team to find a solution to a more significant issue the world is currently facing thanks to his high-level explanation, study results, and real-world data. The newly opened Cancer Center at the University of Maiduguri Teaching Hospital (UMTH) would go a long way toward reducing the amount of regular medical travel that Nigerians engage in. The Cancer Center is the only facility in Nigeria with four bunkers and cutting-edge medical equipment to ensure that cancer patients receive top-notch care.

Recalls that Alh. Mamman Mamuda, the Permanent Secretary of the Federal Ministry of Health, said of the UMTH during the inspection of projects completed in the hospital that other cancer centers across the nation “are not up to the standard” of the UMTH Cancer Center and lack the capacity. From what I have observed on the ground, I can conclude that the UMTH is prepared to put an end to medical tourism in Nigeria, he claimed. We have already begun planning ways to make the UMTH a recipient of the Federal Government of Nigeria’s Cancer Support Fund.
The Cancer Center, which cost more than N5 billion to build, has the newest medical facilities in Sub-Saharan Africa, according to the Chief Medical Director (CMD) of the UMTH, Prof. Ahmed Ahidjo. He also noted that the goal of the UMTH is to prevent any medical issues from being referred to outside facilities, such as the Epic Hospital in the North East Region. We have two linear accelerators, two brachytherapists, and four bunkers here. We are bringing the first linear accelerators into Nigeria with the Nectar Infinite. The second one, HD Versa, for which the Federal Ministry of Health recently completed the purchase procedure for us, is the first to enter sub-Saharan Africa and the most recent method used globally.

Alongside the Permanent Secretary, Director of Hospital Services Dr. Adebinpe Adebiyi praised the Cancer Center as one of the greatest in the nation and claimed that “it is beating the trends” set by other centers before it. Dr. Adebiyi disclosed that the management of UMTH has given the issue of staffing the new cancer center great priority, noting that the capacity building of professionals to staff the center has been completed. “When Nigerians travel overseas and encounter other Nigerians, they are treated with respect. Why are they not able to treat Nigerians here? It was her.
In Borno State, the CMD is being praised for the several initiatives he is putting in place to make Maiduguri a tourism hub for health in Nigeria, especially with the country’s largest cancer center and cutting-edge medical technology. The move and encouragement needed from the previous administration to the current one, under President Bola Ahmed Tinubu, is to have more federal presence at the University of Maiduguri Teaching Hospital through activities that would promote bigger dreams for a better health solution in Nigeria.
Special Report-UMTH: Looking at the Cancer Center Under Professor Ahidjo’s Led Management Team (3)

Health
Investigation: Why Barrister Hamza Nuhu Dantani should apologize to UMTH over his claims; his father’s case—”Prostate Cancer at Stage Four”—was a hopeless situation despite the fact that he was attended to by one of the best urologists.

Investigation: Why Barrister Hamza Nuhu Dantani should apologize to UMTH over his claims; his father’s case—”Prostate Cancer at Stage Four”—was a hopeless situation despite the fact that he was attended to by one of the best urologists.
By: Dr. James Bwala
The recent public allegations made by Barrister Hamza Nuhu Dantani against the University of Maiduguri Teaching Hospital (UMTH) concerning the treatment of his late father have stirred significant controversy and raised critical questions about professional conduct, medical ethics, and the responsibilities of legal practitioners in public discourse. While empathy for the loss of a family member is natural, it is vital that claims made in the public domain, especially those affecting reputable institutions, are founded on verified facts and conveyed with professionalism. After thorough investigation and engagement with UMTH officials and medical experts, it becomes evident that Barrister Dantani’s assertions lack merit and, more importantly, that his conduct in this matter falls short of the standards expected from a legal professional. Consequently, Barrister Hamza Nuhu Dantani should publicly apologize to UMTH for the unsubstantiated nature of his claims and the undue damage inflicted upon the institution’s reputation.
To appreciate fully why an apology is necessary, one must first understand the medical circumstances surrounding the late Alhaji Dantani’s admission to UMTH. Medical records and testimonies indicate that the elder Dantani was admitted at an advanced stage of prostate cancer—specifically stage four—in February 2026. This is a critical point in the disease’s progression wherein the cancer has metastasized extensively, generally rendering curative treatment unattainable regardless of the quality of care provided. Globally, stage four prostate cancer presents a near-hopeless prognosis, demanding palliative rather than curative efforts to maximize quality of life. It is misleading, therefore, to interpret the outcome as resultant from negligence or substandard care following Alhaji Dantani’s demise on March 31, 2026.
READ ALSO: https://newsng.ng/the-complex-reality-of-healthcare-a-perspective-on-the-university-of-maiduguri-teaching-hospital-and-the-loss-experienced-by-barrister-nuhu-dantani-hamza/
My findings also revealed that the late patient’s care was overseen by Professor Hassan Dogo, a urologist of outstanding repute both within and beyond Nigerian medical circles. Professor Dogo’s involvement underscores the level of expertise committed to the patient’s management. The hospital’s Chief Medical Director, Professor Ahmed Ahidjo, personally intervened to ensure that the Dantani family had access to the best possible care, even offering private quarters within the hospital should general wards be unavailable. This proactive and compassionate response demonstrates the hospital’s commitment to patient welfare and contradicts any insinuations of neglect or unprofessionalism.
The decision by Barrister Dantani to publicly air grievances on social media and through petitions before fully engaging with hospital authorities exemplifies unprofessional conduct unbecoming of a lawyer. As an officer of the court, a barrister bears the responsibility not only to uphold the law but also to maintain decorum and integrity in all public interactions. Recklessly disseminating claims without validation jeopardizes the credibility of the legal profession and undermines public trust in medical institutions that serve critical societal needs. In this instance, such premature public accusations inflicted reputational harm on UMTH, an institution known for its high standards and dedicated service.
READ ALSO: https://newsng.ng/the-complex-reality-of-healthcare-a-perspective-on-the-university-of-maiduguri-teaching-hospital-and-the-loss-experienced-by-barrister-nuhu-dantani-hamza/
In addition to institutional harm, the manner in which Barrister Dantani handled the situation reflects poorly on the principles of due diligence and respectful dialogue. Rather than pursuing direct communication with UMTH management to clarify concerns, he resorted to externalizing grievances, thereby exacerbating tensions. The fact that members of the Dantani family subsequently contacted the hospital to express regret over the son’s approach confirms that the claims were disproportionately escalated. This sequence of events highlights the need for measured responses grounded in factual understanding, especially when involving matters as sensitive as terminal illness.
It is also essential to contextualize the nature of cancer prognosis within the public discourse. Awareness that advanced-stage cancers often defy medical intervention is critical in mitigating misplaced blame on healthcare providers. By advancing inaccurate narratives, public figures risk fostering distrust in healthcare systems, potentially discouraging others from seeking timely medical attention. Barrister Dantani, equipped with professional training and access to legal and investigative resources, had an obligation to ascertain the veracity of the situation before turning to public condemnation.
READ ALSO: https://newsng.ng/the-complex-reality-of-healthcare-a-perspective-on-the-university-of-maiduguri-teaching-hospital-and-the-loss-experienced-by-barrister-nuhu-dantani-hamza/
Some people out there might argue that the family’s grief justified Barrister Dantani’s public expressions or that highlighting perceived gaps in patient care could promote systemic improvements. While grief is deeply personal and valid, it does not justify undermining established protocols for dispute resolution or tarnishing reputations without substantiation. Constructive criticism aimed at improving health services is best channeled through official and collaborative frameworks rather than adversarial and public confrontations lacking evidence. Moreover, in this case, available information strongly suggests that the hospital maintained high standards of care, negating the premise for such allegations.
I believe the intersection of professional responsibility, respect for institutional integrity, and empathetic understanding of medical realities informs the necessity for Barrister Hamza Nuhu Dantani to issue an unambiguous apology to UMTH. His premature and unfounded public criticisms unfairly discredited the hospital, disregarding the complex and tragic nature of late-stage prostate cancer and the commendable efforts of its medical staff. An apology would not only restore dignity to UMTH but also reaffirm the ethical standards expected of legal practitioners. Moving forward, this episode should serve as a reminder of the importance of prudence, respect, and factual accuracy in public discourse—especially when lives and legacies are involved. Only through such conscientious conduct can professional integrity and public trust be preserved for the benefit of society at large. This is my take following the unfortunate incident.
* James Bwala, PhD, writes from Abuja.
Investigation: Why Barrister Hamza Nuhu Dantani should apologize to UMTH over his claims; his father’s case—”Prostate Cancer at Stage Four”—was a hopeless situation despite the fact that he was attended to by one of the best urologists.
Health
The Complex Reality of Healthcare: A Perspective on the University of Maiduguri Teaching Hospital and the Loss Experienced by Barrister Nuhu Dantani Hamza
The Complex Reality of Healthcare: A Perspective on the University of Maiduguri Teaching Hospital and the Loss Experienced by Barrister Nuhu Dantani Hamza
By: Dr. James Bwala
The recent public outburst by Barrister Nuhu Dantani Hamza, a lawyer based in Abuja, over the demise of his father at the University of Maiduguri Teaching Hospital (UMTH) has sparked intense discussions about the quality of healthcare services provided by the institution. While it is entirely understandable to empathize with Barrister Hamza’s profound grief and frustration following such a personal loss, it is crucial to examine the context and facts surrounding this case before drawing conclusions about institutional failure.
My parents are no more. I nursed them at the same UMTH before their demise, and so have many others. Death comes when it comes. We never blame it on any health institution or person; rather, we return glory to God Almighty, who gives and takes. I therefore contend that the death of an individual patient, however painful, does not equate to a wholesale failure of a healthcare institution like UMTH, particularly when thousands of other patients have reported satisfactory experiences. By exploring the nuances of medical care, the realities of patient outcomes, the specific privileges associated with amenity wards, and public testimonies about UMTH, I wish to offer a balanced and reasoned perspective on this delicate matter.
READ ALSO: https://newsng.ng/2027-who-owns-the-adc-presidential-ticket/
First and foremost, it is important to acknowledge the deep sorrow and empathy owed to Barrister Hamza and his family. The passing of a loved one, especially a parent, represents one of life’s most traumatic experiences. Barrister Hamza’s passionate response—the “threatening hell and storms” directed at UMTH—reflects a natural human reaction to loss, anger, and perhaps perceived helplessness. Compassion compels us to stand with him in mourning. Yet, simultaneously, grief may cloud judgment, leading to an oversimplification of complex realities involved in healthcare delivery and medical outcomes. Emotionally charged reactions, though valid as expressions of pain, should not be conflated with objective evaluations of medical institutions.
A fundamental truth often overlooked in public debates about hospital performance is that death, despite advances in modern medicine, remains an inevitable aspect of human existence. No healthcare system or institution, regardless of prestige or resources, can guarantee survival in every circumstance; else, our former president, Muhammadu Buhari, would not have died in a London hospital given his resources and care. Patients admitted to hospitals frequently face serious, sometimes terminal conditions. Even the best-equipped medical facilities staffed by highly trained specialists encounter cases where, despite exhaustive interventions, outcomes are unfavorable due to the nature and severity of the illness.
READ ALSO: https://newsng.ng/2027-who-owns-the-adc-presidential-ticket/
In the case of Barrister Hamza’s father, who was admitted sometime in February 2026 and passed away on March 31, 2026, medical terminology used by the bereaved son indicates a level of familiarity with hospital procedures. This familiarity suggests an awareness that mortality is not necessarily synonymous with negligence or incompetence. Indeed, medical professionals operate within biological limits and uncertainties inherent to health and disease. Appreciating this reality is vital to forming a fair assessment of any healthcare institution.
An important detail in Barrister Hamza’s account is the admission of his father to amenity ward “B” at UMTH. Amenity wards are generally designated areas offering enhanced comfort, privacy, and specialized attention compared to standard hospital wards. Admission to such a ward typically implies that the patient was accorded preferential treatment, access to superior facilities, and closer monitoring by the medical team. This status inherently involves higher costs but often translates into more personalized and comprehensive care.
READ ALSO: https://newsng.ng/2027-who-owns-the-adc-presidential-ticket/
Therefore, the fact that the deceased was treated in an amenity ward refutes any simplistic claim that he was neglected or denied proper medical attention. On the contrary, this designation underscores the level of attention paid to his well-being, reinforcing the argument that the hospital provided a distinctive standard of care. Knowledgeable observers understand that amenity wards symbolize privilege within hospital frameworks and are designed to maximize patient comfort and oversight.
To pass judgment on UMTH based solely on a single outcome risks ignoring the broader picture of the hospital’s service record. Since 2000, when I began reporting on healthcare in Nigeria, I am aware that journalists and healthcare observers covering the UMTH beat have documented a wide spectrum of patient experiences, ranging from stories of recovery and gratitude to those marked by sorrow and regret. This is a universal truth across all hospitals that some patients will unfortunately succumb to their illnesses. However, the existence of negative outcomes does not negate the fact that many patients receive effective treatment and leave the institution restored to health.
READ ALSO: https://newsng.ng/2027-who-owns-the-adc-presidential-ticket/
In the Nigerian context, and specifically within Borno State and its environs, UMTH has garnered numerous testimonials from patients who have benefited from its care. These affirmations are often overshadowed in public discourse by the louder voices of criticism, yet they constitute a vital counterbalance. A significant number of patients not only recover but actively return to express their thanks for the competent and compassionate care they received. Such accounts attest to the hospital’s capacity to deliver quality healthcare amidst challenging circumstances.
The discourse surrounding Barrister Hamza’s post also illuminates a commendable community effort to defend UMTH’s reputation. One notable example is Alhaji Modu Kellu, identified as a product of UMTH, who publicly vouched for the institution on social media. His defense carries weight as a direct beneficiary of the hospital’s healthcare services, offering an insider’s perspective that challenges unequivocal assertions of negligence.
READ ALSO:https://newsng.ng/2027-who-owns-the-adc-presidential-ticket/
The presence of such voices is critical in any balanced public debate. They demonstrate that the hospital inspires loyalty and trust among certain segments of the population. These defenders highlight the need to differentiate between isolated tragedies and systemic failures. In the absence of evidence pointing conclusively to malpractice or negligence, a hospital’s overall reputation must be preserved to maintain public confidence and morale among healthcare workers.
While defending UMTH’s record is essential, it is equally important to advocate for transparent and objective inquiry into any incidents that cause distress or raise questions. Barrister Hamza’s case should prompt careful review and, if warranted, constructive reforms aimed at improving patient safety and hospital responsiveness. Such scrutiny should be conducted through established medical channels rather than social media denunciations alone. This approach ensures fairness to the institution while honoring the rights and concerns of bereaved families.
READ ALSO: https://newsng.ng/2027-who-owns-the-adc-presidential-ticket/
Constructive dialogue among healthcare providers, patients’ families, regulatory bodies, and the media fosters mutual understanding and continuous improvement. It enables hospitals like UMTH to address potential shortcomings without suffering unjust reputational damage. Equally, it empowers families to seek redress and closure within appropriate frameworks, mitigating the emotional turbulence accompanying loss.
The emotional narrative shared by Barrister Nuhu Dantani Hamza regarding his father’s death at UMTH warrants heartfelt sympathy and respect. However, his story should not be construed as definitive evidence of UMTH’s failure. The privilege of admission to an amenity ward, coupled with thousands of positive patient outcomes over decades, illustrates that UMTH is a capable institution committed to delivering quality healthcare despite inherent limitations.
READ ALSO: https://newsng.ng/2027-who-owns-the-adc-presidential-ticket/
Death, a universal eventuality, does not tarnish the dedication of healthcare professionals nor invalidate successful recoveries experienced by many others. Public defenders of UMTH, including appreciative former patients, reinforce that the hospital maintains a commendable standard of care. Going forward, balanced perspectives, objective investigations, and constructive engagement will remain essential to uphold both patient rights and institutional integrity.
Ultimately, healthcare is a domain marked by complexity, uncertainty, and humanity’s collective endeavor to alleviate suffering. It demands from us both compassion for grieving individuals and reasoned judgment when assessing the performance of medical institutions. By holding these twin principles in tension, we honor both the memory of those lost and the ongoing mission of hospitals like the University of Maiduguri Teaching Hospital.
* James Bwala, PhD, writes from Abuja.
The Complex Reality of Healthcare: A Perspective on the University of Maiduguri Teaching Hospital and the Loss Experienced by Barrister Nuhu Dantani Hamza
Health
UMTH: When VP Kashim Shettima acknowledges Ahidjo and hospital staff for their services to victims of Maiduguri bomb blasts

UMTH: When VP Kashim Shettima acknowledges Ahidjo and hospital staff for their services to victims of Maiduguri bomb blasts
By: Dr. James Bwala
Nigeria’s Vice President, Kashim Shettima, made a commendable visit to the University of Maiduguri Teaching Hospital, UMTH, where he continued with the message of hope for the resilient people of Borno State following the tragic bomb blast that occurred on Monday. His acknowledgment of Professor Ahmed Ahidjo and his team for their dedicated service to the victims highlights not only the resilience of the medical community in times of crisis but also the importance of efficient healthcare systems in mitigating the impact of violence and tragedy. He also observed the critical role that healthcare institutions and professionals play in society, particularly in regions plagued by conflict, and the necessity of supporting such institutions through recognition, resources, and policy for effective services.

The recent bombing incident serves as a somber reminder of the constant threats faced by communities in Borno State and much of northeastern Nigeria. While the incident itself is tragic, the response from the healthcare sector illustrates hope and human compassion in the face of adversity. The vice president’s visit to the hospital is more than just a gesture; it underscores the significance of swift medical intervention and the tremendous effort undertaken by healthcare workers who bravely confront the consequences of violence daily.
READ ALSO: https://newsng.ng/maiduguri-bomb-blast-in-time-of-tragedies-let-us-also-understand-vp-kashim-shettimas-position/
Professor Ahmed Ahidjo and his team’s prompt response to the devastation caused by the bombing is worthy of praise. Their ability to stabilize the condition of the victims amidst chaos demonstrates professionalism and commitment to life-saving practices. In an environment where resources may be stretched thin and pressures high, the performance of healthcare teams becomes even more vital. These professionals often work under challenging conditions, yet their determined spirit and compassion can significantly affect recovery rates and overall patient outcomes.

The vice president’s expression of gratitude towards the hospital staff reflects a broader understanding of the interconnectedness of governance and healthcare provision. By publicly acknowledging the hard work of medical personnel, government officials can foster a culture of appreciation and respect for the healthcare profession. Such recognition can have far-reaching benefits, motivating current healthcare professionals and attracting aspiring medical practitioners to the field. This encouragement is essential, especially in regions like Borno, where skilled healthcare providers are desperately needed to combat both the immediate health crises and the long-term impacts of violence.
READ ALSO: https://newsng.ng/maiduguri-bomb-blast-in-time-of-tragedies-let-us-also-understand-vp-kashim-shettimas-position/
UMTH’s capacity to effectively aid victims of violent attacks raises crucial questions about healthcare infrastructure in Nigeria. While the University of Maiduguri Teaching Hospital has demonstrated its capability, the sustainability and expansion of such services are necessary for ongoing success. Government investment in healthcare infrastructure is imperative. Targeted funding, training programs, and resources need to be allocated to ensure hospitals can provide comprehensive and timely care, especially in areas prone to conflict. This is not merely a reactive measure; it is proactive engagement that can fortify communities against future tragedies.

In the context of this discussion, it is essential to consider the implications of government policies on healthcare. The vice president’s visit reinforces the need for consistent governmental support of healthcare institutions. Policies that prioritize healthcare funding, facilitate access to medical supplies, and promote the welfare of healthcare workers can lead to improved health outcomes. Furthermore, these policies must address the root causes of the violence that leads to such devastating incidents, recognizing that peace and stability are integral to health and well-being.
READ ALSO: https://newsng.ng/maiduguri-bomb-blast-in-time-of-tragedies-let-us-also-understand-vp-kashim-shettimas-position/
The compassion shown by Vice President Shettima in praying for the victims’ recovery emphasizes the human aspect of political leadership. In a nation where trust in government can sometimes wane, leaders who show empathy and personal investment in their citizens’ welfare can bridge gaps and build stronger connections within communities. This symbolism of care and hope in leadership can mobilize public support, encouraging citizens to engage collaboratively with their governments to improve local conditions.

It is also crucial to highlight the ongoing psychological impact of violence on affected populations. Beyond the physical injuries sustained in such attacks, many victims experience deep psychological scars that require attention and specialized care. Healthcare institutions must evolve to include mental health support services alongside traditional medical treatment. The response from hospitals like the University of Maiduguri Teaching Hospital should extend into mental health initiatives to support victims in their recovery journey holistically.
READ ALSO: https://newsng.ng/maiduguri-bomb-blast-in-time-of-tragedies-let-us-also-understand-vp-kashim-shettimas-position/
In contemplating the significance of the vice president’s visit, we should consider how this moment can be leveraged to initiate broader discussions about healthcare reform in Nigeria. Advocacy for mental health resources, trauma-informed care, and community health capacity-building are all essential components that must be prioritized. The partnership between government, healthcare providers, and communities can create a robust support system that not only addresses immediate crises but also enhances long-term community resilience.

Vice President Kashim Shettima observed that support for healthcare professionals in Nigeria goes beyond mere praise, stating that these individuals require access to continuous education, emotional support, and adequate compensation for their work. Investing in their development ensures that they can provide the highest quality of care, which is essential in crisis situations. Indeed, when healthcare workers are equipped with the right tools and knowledge, their effectiveness during emergencies increases dramatically, thereby saving lives and improving recovery outcomes.
READ ALSO: https://newsng.ng/maiduguri-bomb-blast-in-time-of-tragedies-let-us-also-understand-vp-kashim-shettimas-position/
The commendation given by Vice President Kashim Shettima to Professor Ahmed Ahidjo and his team at the University of Maiduguri Teaching Hospital serves as a powerful testament to the critical role of healthcare in society, especially in areas impacted by conflict. The prompt action taken by medical personnel in response to the bomb blast exemplifies courage and dedication that deserves recognition and support. However, it is imperative to build on this foundation by advocating for robust healthcare policies, investing in infrastructure and personnel training, and fostering community engagement.

Through these concerted efforts, Nigeria can cultivate a healthcare system that not only responds effectively to emergencies but also restores hope, promotes healing, and strengthens communities in times of need. It is a call to action for every citizen, policymaker, and healthcare professional to unite in bolstering the foundations of our healthcare system, ensuring that we are prepared for whatever challenges lie ahead.
* James Bwala, PhD, writes from Maiduguri.
UMTH: When VP Kashim Shettima acknowledges Ahidjo and hospital staff for their services to victims of Maiduguri bomb blasts

Zulum meets NPA’s mgt in Lagos, wants Borno’s export capabilities scaled up

Giwa detention facility completes 1,450 terrorism cases, moves 500 suspects for trial

How Nigeria’s Frontline Troops Are Fed, Managed, and Monitored Amid Social Media Controversy

Roger Federer’s Shock as DNA Results Reveal Myla and Charlene Are Not His Biological Children

THE PLIGHT OF FARIDA

FAILED COUP IN BURKINA FASO: HOW TRAORÉ NARROWLY ESCAPED ASSASSINATION PLOT AMID FOREIGN INTERFERENCE CLAIMS
-
 News2 years ago
News2 years agoRoger Federer’s Shock as DNA Results Reveal Myla and Charlene Are Not His Biological Children
-
Opinions4 years ago
THE PLIGHT OF FARIDA
-
 News1 year ago
News1 year agoFAILED COUP IN BURKINA FASO: HOW TRAORÉ NARROWLY ESCAPED ASSASSINATION PLOT AMID FOREIGN INTERFERENCE CLAIMS
-
 News2 years ago
News2 years agoEYN: Rev. Billi, Distortion of History, and The Living Tamarind Tree
-
 Opinions4 years ago
Opinions4 years agoPOLICE CHARGE ROOMS, A MINTING PRESS
-
 ACADEMICS2 years ago
ACADEMICS2 years agoA History of Biu” (2015) and The Lingering Bura-Pabir Question (1)
-
 Columns2 years ago
Columns2 years agoArmy University Biu: There is certain interest, but certainly not from Borno.
-

 Opinions2 years ago
Opinions2 years agoTinubu,Shettima: The epidemic of economic, insecurity in Nigeria